Est.1979
Providing Integrated Research Solutions in Preclinical Biology

A potential missing information in cancer treatment may be an integrated accurate dosing approach that tailors to patient’s tumor characteristics, as well as the extent of drug penetration in tumor tissue. In current dose escalation study design approaches, a correlation is sought between treatment dosage or systemic (plasma) exposure and treatment response. Most often, drugs are assumed to distribute relatively homogeneously in the tumor tissue. However, distribution of drugs into tumor tissue is in fact highly variable and may not correlate with dose or plasma concentrations. Such variability of drug penetration into tumor tissues may result in suboptimal treatment responses and yet its significance is often neglected.
Thus, an important parameter in therapeutically accurate dosing is drug tumor penetration, which can be assessed by measuring accessibility of the target and drug penetration in tumors at macroscopic and/or microscopic levels. At the macroscopic level, drug penetration is often heterogeneous within one single tumor lesion and even more so across different metastatic sites in the same patient. At the microscopic level, sanctuary sites may result in heterogeneity in drug concentrations leading to a proportion of neoplastic cells not receiving the required therapeutic dose. Anticancer drug distribution will be investigated at four levels, in the context of drug accessibility and downstream pharmacologic effects (Figure 1), bridging the gap between drug dose and the pharmacological link with a solid tumor’s clinical outcome.
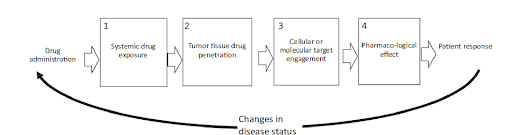
Figure 1 The pathway of drug administration to the tumor response is affected by tumor drug penetration at four levels: (1) the systemic level (the concentration of the drug in the blood pool, which determines how much of the drug is available for tumor penetration), (2) the tissue level (e.g., is the drug able to distribute throughout the tumor tissue, as influenced by the tumor microenvironment), (3) the cellular or molecular engagement level (where the drug is able to engage and interact with its target at the cellular/molecular level, a proximal or direct measure of drug mechanism of action), and (4) the expression of pharmacological activity following target engagement (a distal or indirect measure of drug pharmacodynamics). All these levels will be affected by responses to treatment (bottom).
Here, we will focus on the state-of-the-art tools, including imaging techniques that provide patient-specific information on drug accessibility at the tumor tissue level, target binding, and downstream pharmacology in the context of precision dosing. Although these four drug distribution levels resemble the “three pillars of survival” framework, described in the literature, that includes drug exposure at the target site, target binding, and expression of pharmacological activity, additional consideration of spatial drug distribution in tumor tissue is added here. These four levels and their key considerations are further described below.
Assessment of systemic exposure ensures that the drug achieves a blood concentration during treatment that, in principle, permits optimal penetration and target binding into the tumor tissue, allowing selection of a dose with the best probability to reach the maximal receptor occupancy in the tumor. Ideally, this would be the dose that results in the number of bound target receptors/ proteins in the tumor close to the maximum attainable, which is not always the maximum tolerated dose. Below, we discuss separately assessment of systemic exposure from measurements at the site of action (tumor tissue).
At the tissue level, state-of- the- art techniques may be used to visualize whether the drug is able to homogeneously distribute throughout the tumor. A range of factors (e.g., vascularity, hypoxia, or drug efflux transporters) may influence drug penetration, depending on characteristics of the drug. For immunotherapies, where immune cells are the effectors, the presence of specific immune cells and/or ligands in relation/proximity to tumor cells may affect the immune function and subsequent outcomes. These studies suggest that before onset of an immune response, the presence and colocalization of immune and tumor cells, should be assessed, in addition to drug tissue penetration. Changes in the tumor microenvironment in response to drug treatment can be investigated. Last, for small molecules, the free fraction of the drug (i.e., the pharmacologically active fraction) may be different in tissues vs. the circulation, and, therefore, whenever possible, total and free drug concentrations should be measured.
At the cellular/molecular level, it is possible to assess the presence and accessibility of the target in the right conformation to allow drug binding (i.e., target engagement). As such, drug binding and target availability should be assessed within and across tumor lesions. Furthermore, for some drugs, it is important to assess temporal changes in drug-target engagement. For example, when drug binding results in target internalization and the pharmacologic effect causes target downregulation or upregulation.
Biomarkers that reflect downstream disease cascading effects or treatment effects can also be measured through target binding at the site of action. These distal measurements of pharmacodynamics (PDs) can indirectly demonstrate that sufficient levels of target modulation are being achieved at the site of action, in addition to providing a bridge toward quantification of drug efficacy and/or resistance.
As mentioned previously, drugs need to achieve systemic concentrations in the blood that permit adequate penetration and target binding into the tumor tissues. Assessment of drug concentrations in blood or plasma alone (plasma pharmacokinetics (PKs)) may provide valuable information to guide drug dosing. PKs can be influenced by factors related to the patient, such as age, body weight, activity of drug transporters and metabolizing enzymes, and renal or liver function. Furthermore, these plasma PK profiles can be profoundly different depending on the drug dose administered to the patient. At a low dose, nontarget specific (e.g., receptor in liver) or nontumor but specific (e.g., circulating target in blood) binding may decrease the drug’s systemic exposure, leading to less drug target binding at the tumor site (the so-called antigen sink). Higher doses may saturate the nonspecific binding sites, and lead to relatively high, non-dose-proportionate, increases in systemic exposure compared to low doses, an effect called target-mediated drug disposition (TMDD). Therefore, evidence of nonlinear clearance by assessment of plasma PK profiles of monoclonal antibodies and other high affinity drugs can sometimes be used as a tool to predict the maximum binding capacity of the accessible drug target.
State-of- the-art tools can be used to assess systemic exposure. During drug development, plasma PK profiles are routinely assessed using techniques, such as liquid chromatography mass spectrometry (LC-MS), for small molecules or immunoassays for monoclonal antibodies. Thus, validated methods for measuring drug concentrations in blood should be available during drug development.
At Dabur Research Foundation, we can dose compounds of interest in xenograft studies and collect all vital organs such as liver, lungs, kidney, heart, spleen, pancreas, brain, muscles, fat, ovary, testes and tumor at specified intervals. Collected organs will be homogenized after addition of water or suitable solvent and analyzed with LC-MS/MS or applicable method to determine compound distribution into tumor and different tissues. This will provide guidance to efficacy studies based on the extent and duration of compound distribution kinetics in various tissues and pharmacological action of compound efficacy to arrive at accurate dosing.
At Dabur Research Foundation, we are supporting all our sponsors by conducting Pharmacokinetic and Tissue Distribution studies in Rats, Mice, Rabbits, guinea pigs to know the newly prepared compound pharmacokinetics and its pharmacodynamics before they enter clinical studies in patients. We have a state of art vivarium facility and bioanalytical laboratory with standard operating procedures to meet global standards. We are AAALAC accredited and GLP facility for conducting animal studies in non-clinical development.